Highly biased meta analysis. Authors originally wrote a highly
biased meta analysis that avoided statistical significance on individual
outcomes with extreme exclusions
Popp, although efficacy was still
seen when looking across all outcomes. Authors modified the protocol published
a short time before, thereby performing a retrospective analysis, clearly
designed to produce a desired outcome.
Authors indicated they would update the analysis but did not
for a very long time. Authors would have been unable to maintain the lack of
statistical significance with the protocol. In this new meta analysis, authors
invented a new method to exclude most studies, thereby producing another
retrospective analysis, again clearly designed to produce the desired
outcome.
Authors included only 14 of 60 studies in the original
analysis. For the update, they include even fewer studies, 11 of 87. A key
method used was excluding studies without confirmation of prospective
registration, however authors violate this to include the Together Trial
twitter.com, which
accounts for 40% of the patients in the extreme subset selected.
In the companion article for the new exclusion methods, authors
note that one indicator for exclusion is if the observed risk reduction is too
large
medrxiv.org, .
The trial resulting in Paxlovid approval would be excluded on this
basis.
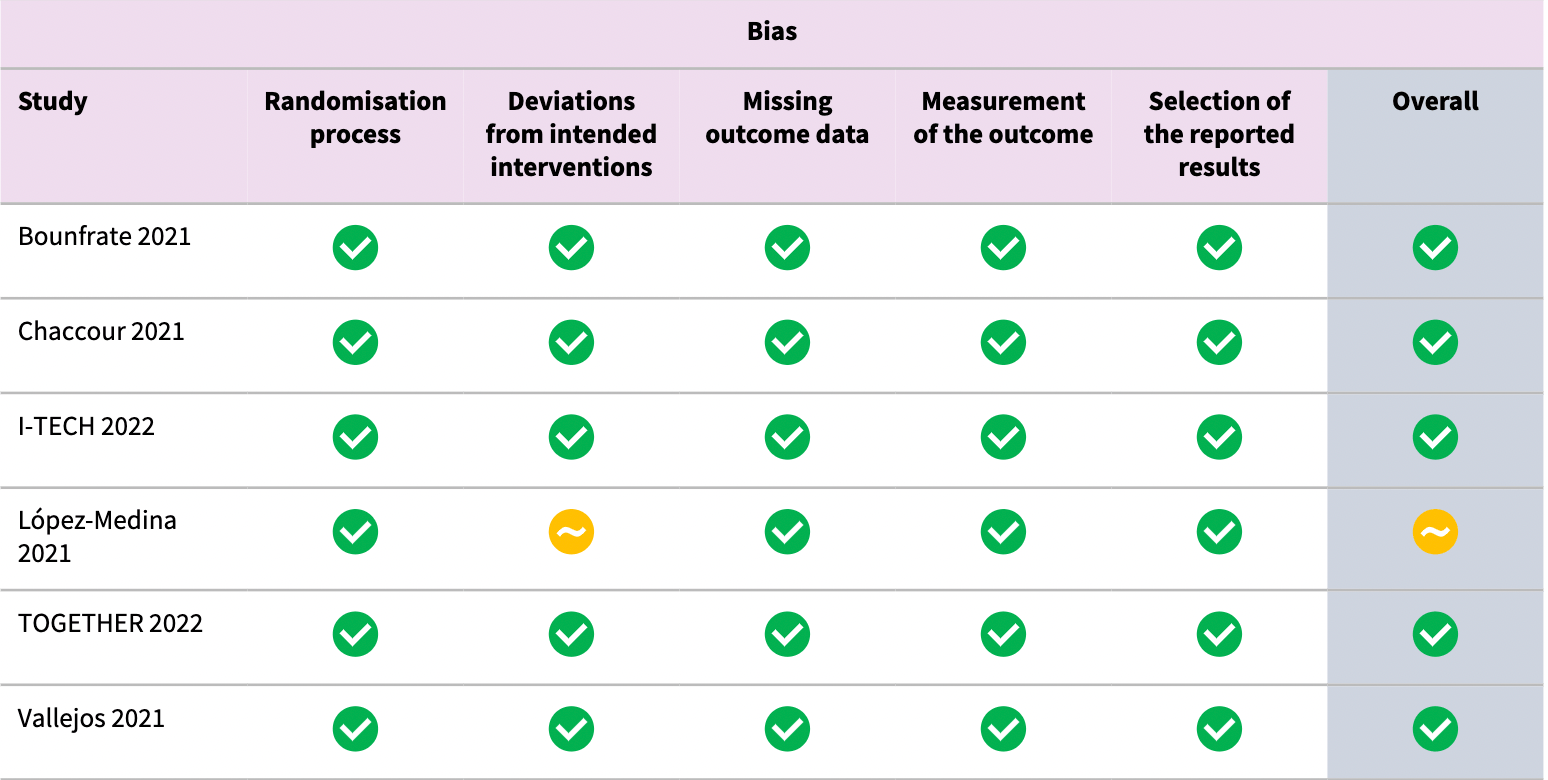
As just one example of extreme bias, authors classify the
Together Trial as low risk of bias. This trial not only has very high risk of
bias, but has very high actual known bias. The trial has refused to release
data despite pledging to, has reported multiple impossible numbers, and had
blinding failure and randomization failure, along with many other issues
Reis.
As another example of extreme bias, the authors avoid reporting
on the 3 prophylaxis RCTs that all reported statistically significant
improvement at the time (as of Jan 2023 there are 4, all showing statistically
significant improvements), by simply deciding not to do so. Authors know that
this shows statistically significant efficacy because they acknowledge
reviewing our analysis.
Notably, the paxlovid analysis from many of the same authors does not do this.
The table shows the inclusion criteria for case results in their paxlovid vs.
ivermectin analyses. Using the paxlovid criteria for ivermectin would show
statistically significant reduction for both cases and clinical symptoms with
ivermectin.
| Paxlovid | Ivermectin |
| Shared Cochrane authors |
Popp, Reis, Metzendorf, Kranke, Meybohm, Skoetz, Weibel |
Popp, Reis, Metzendorf, Kranke, Meybohm, Skoetz, Weibel |
| Prophylaxis inclusion |
PrEP or PEP
PCR/antigen+ @14 days and 6 months
clinical symptoms @28 days and 6 months
|
PEP only
PCR/antigen+ @14 days
clinical symptoms @14 days
|
| Matching studies |
1 showing no significant effect, which was not included Pfizer |
0 |
| Matching studies with paxlovid criteria |
|
4, all showing statistically significant improvements |
The analysis is also very out of date, including trials only up
to April 2022, and including only trials with >1,000 patients since Dec 16,
2021 (yet another cherry-picking mechanism).
With regards to ivmmeta:
- authors claim ivmmeta "states the FLCCC and BIRD as its
resources". This is false, there is no relationship with FLCCC or BIRD.
- author's discussion of pooled estimates is disingenuous.
ivmmeta reports individual outcome results which are the first item discussed
in the abstract. The advantages and disadvantages of pooled estimates are
clearly discussed.
- authors statement that there is no prospective protocol is
highly disingenuous. The ivmmeta protocol was published in November 2020, is
unchanged from the same protocol published in October 2020 used for another
medication, and the same protocol is used for 42 treatments. The ivmmeta
analysis has been updated regularly with the same protocol. In contrast,
authors have published their meta analysis only twice, both times changing the
protocol creating a retrospective analysis. Further, authors have created a
new unique protocol for this treatment.
- authors claim that "there is no assessment of the risk of
bias or the certainty of evidence". This is false, studies are evaluated and
29 are excluded in exclusion analyses. Authors could note that ivmmeta focuses
on actual bias as opposed to theoretical risk of bias. While authors assess
risk of bias, their assessment is implausible, as shown with the example of
the Together Trial above. Note that not only does the Together Trial have
extreme actual bias, the theoretical risk of bias is also extremely high due
to the conflicts of interest and trial design.
See
Popp for many other issues.
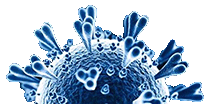
Currently there are
102 ivermectin for COVID-19 studies, showing 49% lower mortality
[35‑60%], 29% lower ventilation
[12‑42%], 35% lower ICU admission
[7‑54%], 34% lower hospitalization
[20‑45%], and 81% fewer cases
[71‑87%].
Popp et al., 21 Jun 2022, preprint, 10 authors.
Ivermectin for preventing and treating COVID-19
Maria Popp, Stefanie Reis, Selina Schießer, Renate Ilona Hausinger, Miriam Stegemann, Maria-Inti Metzendorf, Peter Kranke, Patrick Meybohm, Nicole Skoetz, Stephanie Weibel
Cochrane Database of Systematic Reviews, doi:10.1002/14651858.cd015017.pub3
Analysis 1.1. Comparison 1: Ivermectin for treating COVID-19 in inpatient settings with moderate to severe disease, Outcome Analysis 2.12. Comparison 2: Ivermectin for treating COVID-19 in outpatient settings with asymptomatic or mild disease, Outcome
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Study characteristics
Methods • Trial design: triple-blind RCT with 3 parallel arms, the 2 intervention arms were pooled for this review • Type of publication: pre-proof journal publication • Severity of condition according to study definition: mild disease, defined as not requiring hospitalization or oxygen supplementation • Severity of condition according to WHO scale: 1 to 3 • Time from symptom onset to enrolment (median): overall 4 (IQR 3 to 5.5) days • Comorbidities: any pre-existing condition, obesity, diabetes, cardiovascular disease, respiratory disease • Virus detection performed at baseline (test-positive at baseline): RT-PCR (100%) • Vaccination status: overall 91 (98%) participants without any vaccination • Inclusion criteria: age ≥ 18 years; positivity for SARS-CoV-2 (nasopharyngeal swabs) by RT-PCR; consent to participating in the study and to the processing of personal data; COVID-19 Severity Score < 3; participant able to take oral drugs Cochrane Database of Systematic Reviews • Exclusion criteria: pregnant or lactating women (pregnancy test not required, if doubt person is excluded); people with known central nervous system disease; lack of (or inability to provide) informed consent; receiving dialysis; any severe medical condition with a prognosis of < 6 months; receiving warfarin treatment; receiving antiviral treatment; receiving..
References
Blankenfeld, Kaduszkiewicz, Kochen, Pömsl, Scherer et al., Interleukin-6 blocking agents for treating COVID-19: a living systematic review,
doi:10.1002/14651858.CD013881Deeks, Higgins, Altman, Chapter 10: Analysing data and undertaking meta-analyses
Garegnani, Madrid, Meza, Misleading clinical evidence and systematic reviews on ivermectin for COVID-19, BMJ Evidence Based Medicine
German Awmf Guideline 2021a Kluge, Janssens, Welte, Weber-Carstens, Schälte et al., S3-Guideline -recommendations on Inpatient Treatment of Patients With COVID-19
German Awmf Guideline, None
Goetz, Magar, Dornfeld, Giese, Pohlmann et al., Influenza A viruses escape from MxA restriction at the expense of e icient nuclear vRNP import, Scientific Reports,
doi:10.1038/srep23138González-Canga, None
González-Canga, Sahagún-Prieto, Diez-Liébana, Fernández-Martínez, Vega et al., The pharmacokinetics and interactions of ivermectin in humans, Journal of the American Association of Pharmaceutical Scientists,
doi:10.1208/s12248-007-9000-9Herrmann, Adam, Notz, Helmer, Sonntagbauer et al., COVID-19 induced acute respiratory distress syndrome -a multicenter observational study
Higgins, Lasserson, Chandler, Tovey, Thomas et al., Retraction: Expression of Concern: "Meta-analysis of Randomized Trials of Ivermectin to Treat SARS-CoV-2 Infection, Open Forum Infectious Diseases,
doi:10.1093/ofid/ofab358Izcovich, Peiris, Ragusa, Tortosa, Rada et al., Bias as a source of inconsistency in ivermectin trials for COVID-19: a systematic review. Ivermectin's suggested benefits are mainly based on potentially biased results, Journal of Clinical Epidemiology,
doi:10.1016/j.jclinepi.2021.12.018Karagiannidis, Mostert, Hentschker, Voshaar, Malzahn et al., Case characteristics, resource use, and outcomes of 10,021 patients with COVID-19 admitted to 920 German hospitals: an observational study, Lancet Respiratory Medicine,
doi:10.1016/S2213-2600(20)30316-7Kobayashi, Jung, Linton, Kinoshita, Hayashi et al., Communicating the risk of death from novel coronavirus disease (COVID-19), Journal of Clinical Medicine,
doi:10.3390/jcm9020580Kory, Meduri, Varon, Iglesias, Marik, Review of the emerging evidence demonstrating the e icacy of ivermectin in the prophylaxis and treatment of COVID-19, American Journal of Therapeutics,
doi:10.1097/MJT.0000000000001377Kreuzberger, Hirsch, Chai, Tomlinson, Khosravi et al., SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19, Cochrane Database of Systematic Reviews,
doi:10.1002/14651858.CD013825.pub2Lefebvre, Glanville, Briscoe, Littlewood, Marshall et al., Chapter 4: Searching for and selecting studies
Mikolajewska, Fischer, Piechotta, Mueller, Metzendorf et al., Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement, Cochrane Database of Systematic Reviews,
doi:10.1002/14651858Oran, Topol, The proportion of SARS-CoV-2 infections that are asymptomatic: a systematic review, Annals of Internal Medicine,
doi:10.7326/M20-6976Panahi, Poursaleh, Goldust, The e icacy of topical and oral ivermectin in the treatment of human scabies, Annals of Parasitology
Popp, Kranke, Meybohm, Metzendorf, Skoetz et al., Evidence on the e icacy of ivermectin for COVID-19: another story of apples and oranges, BMJ Evidence Based Medicine,
doi:10.1136/bmjebm-2021-111791Ritchie, Mathieu, Rodés-Guirao, Appel, Giattino et al., Coronavirus pandemic (COVID-19)
Rodríguez-Mega E ; Rothrock ; Rothrock, Weber, Giordano, Barneck, Meta-Analyses do not establish improved mortality with ivermectin use in COVID-19, American Journal of Therapeutics,
doi:10.1038/d41586-020-02958-2Rodríguez-Mega, None
Schünemann, Higgins, Vist, Glasziou, Akl et al., Chapter 14: Completing 'Summary of findings' tables and grading the certainty of the evidence
Singh, Ryan, Kredo, Chaplin, Fletcher et al., Vitamin D supplementation References to other published versions of this review Popp, Cochrane Database of Systematic Reviews,
doi:10.1002/14651858

{kind=link}