Ivermectin for COVID-19
4th treatment shown to reduce risk in
August 2020
Lower risk for mortality, ventilation, ICU admission, hospitalization, recovery, cases, and viral clearance.
No treatment is 100% effective. Protocols
combine complementary and synergistic treatments. * >10%
efficacy in meta analysis with ≥3 clinical studies.
4,000+ studies for
60+ treatments. c19ivm.org
|
| Molnupiravir PANORAMIC Gbinigie, isrctn.com |
Ivermectin PRINCIPLE isrctn.com (B) | |
|---|---|---|
| Investigator | Prof. Chris Butler | Prof. Chris Butler |
| Delay | ≤5 days from onset median 2 days |
≤14 days from onset median unknown |
| Population | 50+ or 18+ w/comorbidities | 18+ (mid-trial change) |
| Treatment | 5 days, 2x per day | 3 days, 1x per day, dose below real-world use |
| Administration | Per recommendation (with or without food) | Directed to take opposite of recommendation for COVID-19 - without food, greatly reducing concentration c19ivm.org, Guzzo |
| Patients | 25,783 | 3,963 (inc. concurrent control) |
| Publication delay | 4 months | 19 months (26 months from expected end) |
| Enrollment | Dec 2021 - Apr 2022 | May 2021 - Jul 2022 |
| Mutagenic | Yes | No |
| Cost | $707 fiercepharma.com | <$1 medrxiv.org |
| Merck profit | >$7.2B sales to date merck.com, estimated $18 to produce theintercept.com | ~$0 (potential, unlikely competitive with low cost manufacturers) |
| Design better for showing efficacy | ||
| Design better for hiding efficacy | ||
| PRINCIPLE trial timeline | |
| Date | Change |
|---|---|
| March 22, 2020 | Inclusion ≤7 days, age 50+ w/comorbidity or 65+. |
| June 16, 2020 | Inclusion changed to ≤14 days. |
| February 14, 2021 | Inclusion changed to 18+ w/COVID dyspnea or comorbidity or 65+ c19ivm.org (C). |
| May 12, 2021 | Ivermectin listed as current intervention in protocol web.archive.org. |
| June 2021 | Ivermectin added according to web site principletrial.org. |
| Jul 12, 2021 | Inclusion changed to 18+ c19ivm.org (D). |
| December 2021 | Anticipated completion of ivermectin arm. |
| December 3, 2021 | Ivermectin arm ends, removed from web site between Dec 2 and Dec 3 twitter.com, web.archive.org (F), web.archive.org (G). |
| December 2021 | No press release or rapid top-tier publication, indicating positive results. |
| December 9, 2021 | Ivermectin added back to web site with claim of pause due to supply issues. |
| December 14, 2021 | Trial does not respond to MedPage Today regarding supply problems. A statement from Merck is dramatically different to their previous position and is consistent with them knowing that a trial they cannot ignore has positive results and them being unsure if they can suppress the results medpagetoday.com. |
| December 25, 2021 | The trial supplier, Edenbridge, denies any supply issue. Prof. Chris Butler declines to comment web.archive.org (H). The trial used standard widely available tablets dailymed.nlm.nih.gov, twitter.com (B). |
| January 14, 2022 | Prof. Paul Little, TSC chair, is removed from the trial in protocol version 13 c19ivm.org (E). The TSC is responsible for reporting ethical issues. |
| January 27, 2022 | Trial paused without explanation c19ivm.org (F). |
| February 11, 2022 | Trial only open intermittently (twice daily between Sunday and Thursday), adding further enrollment delays c19ivm.org (G). |
| July 8, 2022 | Extended ivermectin arm ends web.archive.org (I). |
| July 2022 | No press release or rapid top-tier publication, indicating positive results. |
| June 2, 2023 | Sometime between May 2 and June 2, authors add a note on the web site indicating that, against protocol, they are delaying and will release in a rigorous and transparent way after extended 1 year followup ends in July web.archive.org (J), web.archive.org (K). Note that the analysis code for professional trials is written and tested in advance. |
| November 6, 2023 | Links to the protocol, amendments, and other supporting documents were removed from the web site. |
| December 2023 | Still no results or update. A link was added to a version 14 of the protocol dated August 8, 2022 (after all arms had completed). The link does not work, pointing to an internal University of Oxford site. The latest version available is 13.0, dated January 14, 2022 c19ivm.org (E) (during the ivermectin arm, after the expected end in December 2021). |
| PRINCIPLE trial treatments | |||
| Treatment | Treatment patients | Duration | Results delay |
|---|---|---|---|
| HCQ | 393-408 dcricollab.dcri.duke.edu | 2 months | over 1,300 days principletrial.org (B) |
| Azithromycin thelancet.com | 540 | 6 months | 56 days nihr.ac.uk |
| Budesonide thelancet.com (B) | 1,073 | 4 months | 12 days principletrial.org (C) |
| Doxycycline thelancet.com (C) | 780 | 5 months | 42 days nihr.ac.uk |
| Colchicine bjgp.org | 156 | 3 months | 120 days medrxiv.org (B) |
| Ivermectin | 2,157 | 14 months | 600 days (810 days from ~1,000 per arm enrollment) |
| Favipiravir | ~2,250 | 15 months | over 600 days (over 800 days from ~1,000 per arm enrollment) |
|
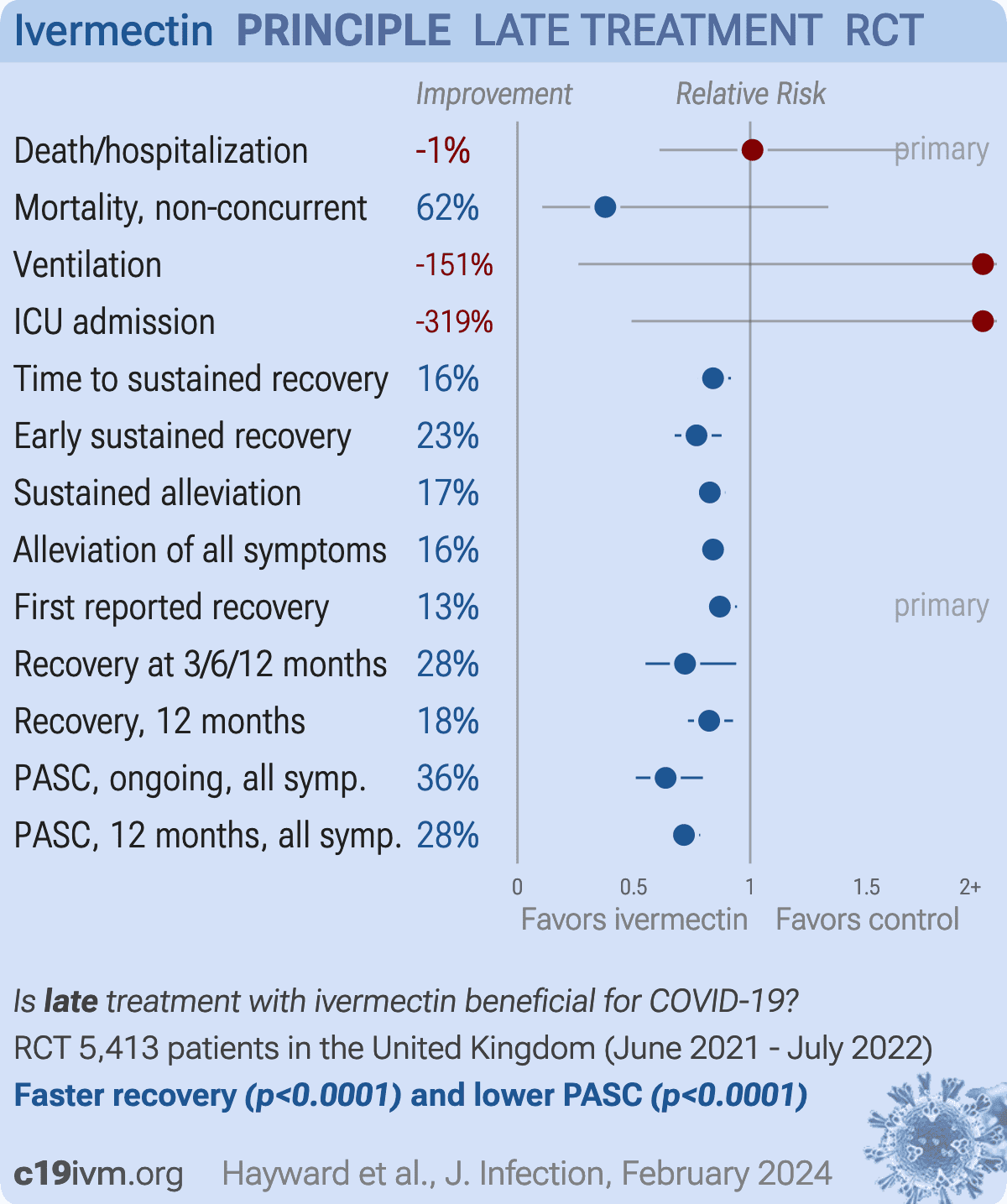
risk of death/hospitalization, 1.0% higher, HR 1.01, p = 0.97, treatment 34 of 2,157 (1.6%), control 27 of 1,806 (1.5%), concurrent and eligible, primary outcome.
|
|
risk of death, 62.3% lower, RR 0.38, p = 0.18, treatment 3 of 2,157 (0.1%), control 12 of 3,256 (0.4%), NNT 436, non-concurrent, authors do not provide details for concurrent deaths.
|
|
risk of mechanical ventilation, 151.4% higher, RR 2.51, p = 0.63, treatment 3 of 2,149 (0.1%), control 1 of 1,801 (0.1%).
|
|
risk of ICU admission, 319.0% higher, RR 4.19, p = 0.23, treatment 5 of 2,149 (0.2%), control 1 of 1,801 (0.1%).
|
|
time to sustained recovery, 16.0% lower, HR 0.84, p < 0.001, treatment 2,157, control 1,806, inverted to make HR<1 favor treatment, concurrent and eligible.
|
|
early sustained recovery, 23.1% lower, HR 0.77, p < 0.001, treatment 2,154, control 1,805, inverted to make HR<1 favor treatment, concurrent and eligible.
|
|
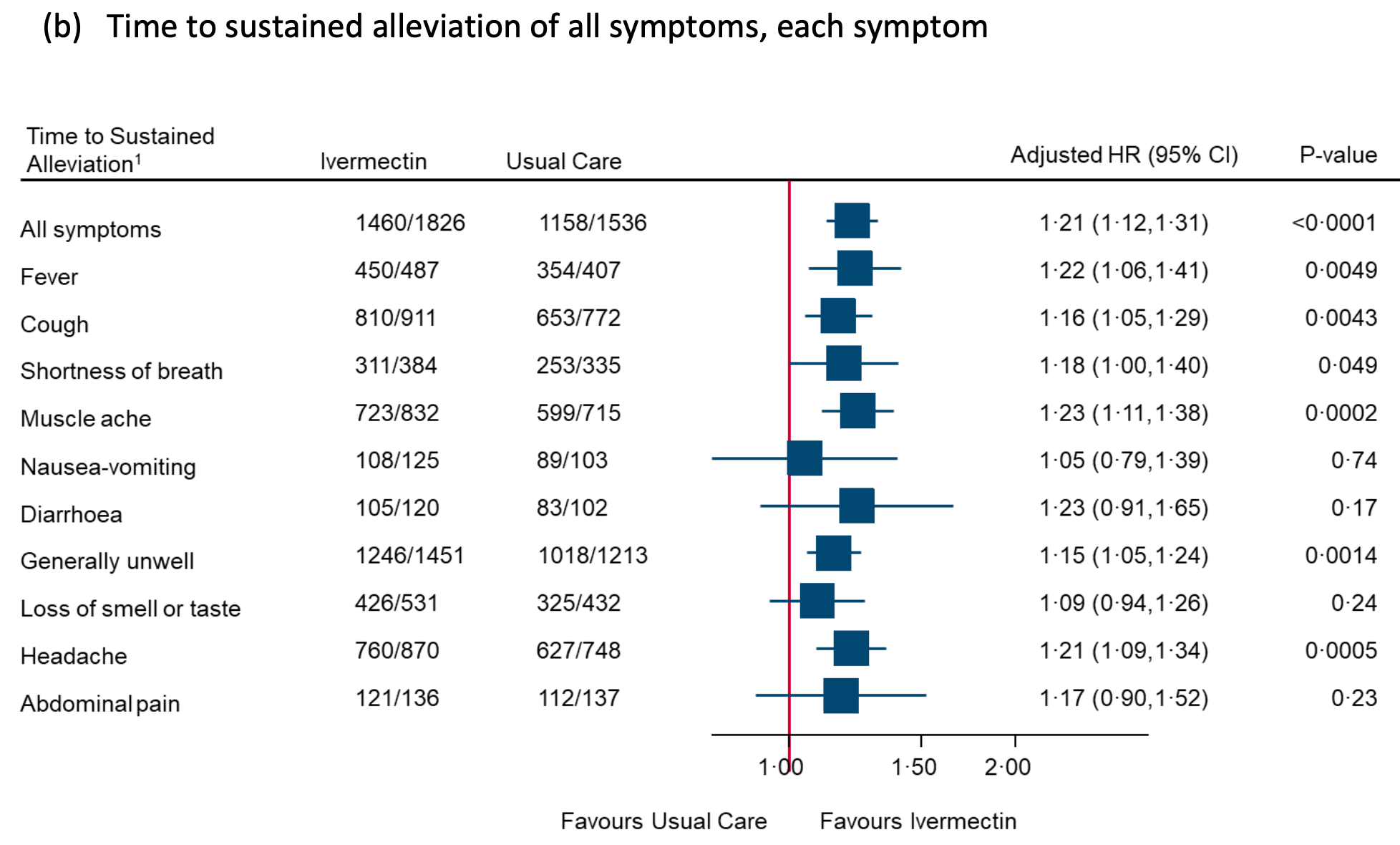
sustained alleviation, 17.4% lower, HR 0.83, p < 0.001, treatment 1,826, control 1,535, inverted to make HR<1 favor treatment, concurrent and eligible.
|
|
alleviation of all symptoms, 16.0% lower, HR 0.84, p < 0.001, treatment 2,154, control 1,805, inverted to make HR<1 favor treatment, concurrent and eligible.
|
|
first reported recovery, 13.0% lower, HR 0.87, p < 0.001, treatment 2,157, control 1,806, inverted to make HR<1 favor treatment, concurrent and eligible, primary outcome.
|
|
no recovery at 3/6/12 months, 28.0% lower, HR 0.72, p = 0.02, treatment 94 of 1,941 (4.8%), control 109 of 1,624 (6.7%), NNT 54.
|
|
risk of no recovery, 17.6% lower, RR 0.82, p = 0.001, treatment 417 of 1,848 (22.6%), control 420 of 1,533 (27.4%), NNT 21, day 365.
|
|
risk of PASC, 36.3% lower, RR 0.64, p < 0.001, treatment 1,886, control 1,567, all symptoms combined.
|
|
risk of PASC, 63.2% higher, RR 1.63, p = 1.00, treatment 2 of 1,507 (0.1%), control 1 of 1,230 (0.1%), ongoing/persistent, fever.
|
|
risk of PASC, 72.7% lower, RR 0.27, p = 0.33, treatment 1 of 1,819 (0.1%), control 3 of 1,489 (0.2%), NNT 683, ongoing/persistent, cough.
|
|
risk of PASC, 50.1% lower, RR 0.50, p = 0.04, treatment 15 of 1,886 (0.8%), control 25 of 1,567 (1.6%), NNT 125, ongoing/persistent, dyspnea.
|
|
risk of PASC, 35.3% higher, RR 1.35, p = 0.74, treatment 5 of 1,808 (0.3%), control 3 of 1,468 (0.2%), ongoing/persistent, chest pain.
|
|
risk of PASC, 25.2% lower, RR 0.75, p = 0.36, treatment 21 of 1,831 (1.1%), control 23 of 1,501 (1.5%), NNT 259, ongoing/persistent, smell.
|
|
risk of PASC, 58.7% lower, RR 0.41, p = 0.42, treatment 2 of 1,821 (0.1%), control 4 of 1,503 (0.3%), NNT 640, ongoing/persistent, diarrhoea.
|
|
risk of PASC, 70.2% lower, RR 0.30, p < 0.001, treatment 10 of 1,739 (0.6%), control 27 of 1,400 (1.9%), NNT 74, ongoing/persistent, headache.
|
|
risk of PASC, 29.8% lower, RR 0.70, p = 0.25, treatment 23 of 1,739 (1.3%), control 27 of 1,433 (1.9%), NNT 178, ongoing/persistent, muscle ache.
|
|
risk of PASC, 47.1% lower, RR 0.53, p = 0.03, treatment 19 of 1,724 (1.1%), control 30 of 1,441 (2.1%), NNT 102, ongoing/persistent, generally unwell.
|
|
risk of PASC, 20.1% lower, RR 0.80, p = 0.19, treatment 66 of 1,876 (3.5%), control 69 of 1,567 (4.4%), NNT 113, ongoing/persistent, fatigue.
|
|
risk of PASC, 28.5% lower, RR 0.72, p < 0.001, treatment 1,513, control 1,238, all symptoms combined.
|
|
risk of PASC, 39.9% lower, RR 0.60, p = 0.01, treatment 46 of 1,435 (3.2%), control 51 of 1,136 (4.5%), relatedness (yes + unsure) 9.1% (treatment) 11.2% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, cough.
|
|
risk of PASC, 41.6% lower, RR 0.58, p < 0.001, treatment 96 of 1,513 (6.3%), control 106 of 1,238 (8.6%), relatedness (yes + unsure) 14.4% (treatment) 18.5% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, shortness of breath.
|
|
risk of PASC, 22.2% lower, RR 0.78, p = 0.27, treatment 39 of 1,426 (2.7%), control 36 of 1,117 (3.2%), relatedness (yes + unsure) 7.6% (treatment) 8.4% (control)
, NNT 205, adjusted per study and for relatedness, moderate/major symptoms at 12 months, chest pain.
|
|
risk of PASC, 38.0% lower, RR 0.62, p = 0.02, treatment 46 of 1,427 (3.2%), control 44 of 1,140 (3.9%), relatedness (yes + unsure) 7.7% (treatment) 10.3% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, palpitations.
|
|
risk of PASC, 11.5% higher, RR 1.12, p = 0.52, treatment 77 of 1,403 (5.5%), control 57 of 1,131 (5.0%), relatedness (yes + unsure) 13.2% (treatment) 12.9% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, smell.
|
|
risk of PASC, 36.4% lower, RR 0.64, p = 0.02, treatment 51 of 1,375 (3.7%), control 51 of 1,116 (4.6%), relatedness (yes + unsure) 1.1% (treatment) 1.4% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, taste.
|
|
risk of PASC, 22.1% lower, RR 0.78, p = 0.37, treatment 26 of 1,290 (2.0%), control 25 of 1,057 (2.4%), relatedness (yes + unsure) 4.8% (treatment) 5.3% (control)
, NNT 286, adjusted per study and for relatedness, moderate/major symptoms at 12 months, ear ache.
|
|
risk of PASC, 9.6% higher, RR 1.10, p = 0.73, treatment 37 of 1,325 (2.8%), control 25 of 1,089 (2.3%), relatedness (yes + unsure) 6.7% (treatment) 7.4% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, sore throat.
|
|
risk of PASC, 34.8% lower, RR 0.65, p = 0.12, treatment 24 of 1,308 (1.8%), control 27 of 1,077 (2.5%), relatedness (yes + unsure) 6.0% (treatment) 6.9% (control)
, NNT 149, adjusted per study and for relatedness, moderate/major symptoms at 12 months, hoarse voice.
|
|
risk of PASC, 16.6% higher, RR 1.17, p = 0.42, treatment 60 of 1,341 (4.5%), control 46 of 1,082 (4.3%), relatedness (yes + unsure) 8.3% (treatment) 7.4% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, tinnitus.
|
|
risk of PASC, 34.7% lower, RR 0.65, p = 0.29, treatment 13 of 1,382 (0.9%), control 12 of 1,139 (1.1%), relatedness (yes + unsure) 2.2% (treatment) 3.0% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, vomiting.
|
|
risk of PASC, 46.5% higher, RR 1.46, p = 0.12, treatment 44 of 1,439 (3.1%), control 25 of 1,175 (2.1%), relatedness (yes + unsure) 5.9% (treatment) 5.8% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, abdominal pain.
|
|
risk of PASC, 1.6% lower, RR 0.98, p = 0.95, treatment 33 of 1,416 (2.3%), control 24 of 1,167 (2.1%), relatedness (yes + unsure) 4.4% (treatment) 5.1% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, diarrhoea.
|
|
risk of PASC, 43.8% higher, RR 1.44, p = 0.23, treatment 30 of 1,417 (2.1%), control 17 of 1,160 (1.5%), relatedness (yes + unsure) 4.5% (treatment) 4.6% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, reduced appetite.
|
|
risk of PASC, 89.8% higher, RR 1.90, p = 0.27, treatment 11 of 1,375 (0.8%), control 4 of 1,129 (0.4%), relatedness (yes + unsure) 1.8% (treatment) 2.2% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, weight loss.
|
|
risk of PASC, 41.3% lower, RR 0.59, p < 0.001, treatment 89 of 1,287 (6.9%), control 94 of 973 (9.7%), relatedness (yes + unsure) 13.2% (treatment) 16.2% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, anxiety.
|
|
risk of PASC, 38.6% lower, RR 0.61, p < 0.001, treatment 95 of 1,298 (7.3%), control 92 of 992 (9.3%), relatedness (yes + unsure) 13.7% (treatment) 17.4% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, depression.
|
|
risk of PASC, 49.0% lower, RR 0.51, p < 0.001, treatment 129 of 1,376 (9.4%), control 143 of 1,105 (12.9%), relatedness (yes + unsure) 19.6% (treatment) 27.3% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, brain fog.
|
|
risk of PASC, 32.9% lower, RR 0.67, p = 0.08, treatment 37 of 1,187 (3.1%), control 33 of 874 (3.8%), relatedness (yes + unsure) 7.1% (treatment) 9.2% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, confusion.
|
|
risk of PASC, 41.9% lower, RR 0.58, p < 0.001, treatment 78 of 1,278 (6.1%), control 81 of 964 (8.4%), relatedness (yes + unsure) 12.5% (treatment) 15.7% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, headache.
|
|
risk of PASC, 45.4% lower, RR 0.55, p = 0.001, treatment 53 of 1,254 (4.2%), control 54 of 955 (5.7%), relatedness (yes + unsure) 11.5% (treatment) 15.8% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, dizziness.
|
|
risk of PASC, 73.5% lower, RR 0.27, p = 0.10, treatment 3 of 1,105 (0.3%), control 3 of 802 (0.4%), relatedness (yes + unsure) 0.4% (treatment) 1.1% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, fainting.
|
|
risk of PASC, 38.7% lower, RR 0.61, p = 0.02, treatment 42 of 1,200 (3.5%), control 39 of 894 (4.4%), relatedness (yes + unsure) 7.9% (treatment) 10.7% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, numbness.
|
|
risk of PASC, 42.1% lower, RR 0.58, p < 0.001, treatment 123 of 1,288 (9.5%), control 121 of 982 (12.3%), relatedness (yes + unsure) 13.9% (treatment) 18.5% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, sleeping problems.
|
|
risk of PASC, 11.8% lower, RR 0.88, p = 0.37, treatment 99 of 1,180 (8.4%), control 88 of 967 (9.1%), relatedness (yes + unsure) 15.1% (treatment) 16.1% (control)
, NNT 141, adjusted per study and for relatedness, moderate/major symptoms at 12 months, body pains.
|
|
risk of PASC, 32.2% lower, RR 0.68, p < 0.001, treatment 136 of 1,220 (11.1%), control 146 of 1,034 (14.1%), relatedness (yes + unsure) 16.1% (treatment) 19.0% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, joint pains.
|
|
risk of PASC, 30.2% lower, RR 0.70, p < 0.001, treatment 205 of 1,398 (14.7%), control 209 of 1,181 (17.7%), relatedness (yes + unsure) 24.1% (treatment) 28.3% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, fatigue.
|
|
risk of PASC, 31.9% lower, RR 0.68, p = 0.006, treatment 91 of 1,208 (7.5%), control 89 of 997 (8.9%), relatedness (yes + unsure) 14.5% (treatment) 18.1% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, weakness.
|
|
risk of PASC, 35.9% lower, RR 0.64, p < 0.001, treatment 99 of 1,211 (8.2%), control 107 of 1,002 (10.7%), relatedness (yes + unsure) 14.3% (treatment) 17.4% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, generally unwell.
|
|
risk of PASC, 9.2% lower, RR 0.91, p = 0.81, treatment 16 of 1,066 (1.5%), control 11 of 855 (1.3%), relatedness (yes + unsure) 3.0% (treatment) 3.8% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, fever.
|
|
risk of PASC, 42.4% lower, RR 0.58, p = 0.21, treatment 10 of 1,065 (0.9%), control 11 of 853 (1.3%), relatedness (yes + unsure) 3.0% (treatment) 3.7% (control)
, adjusted per study and for relatedness, moderate/major symptoms at 12 months, rashes.
|
|
risk of PASC, 10.0% lower, RR 0.90, p = 0.62, treatment 47 of 1,090 (4.3%), control 41 of 873 (4.7%), NNT 260, adjusted per study, moderate/major symptoms at 12 months, other.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}